
Research Article / Open Access
DOI: 10.31488/HEPH.179
Two Arm Stratified Pilot Study to Assess the Efficacy of the New Individualized Microcurrent Frequencies (IMF) Programs “Power of 3” in Comparison with Standard Healy Applications in Participants Under COVID-19 Crisis Induced Stress
Marcus Schmieke, Peter Marmann*
Healy GmbH, Darritzer Str. 6, Kränzlin, Germany
*Corresponding author:Dr. Peter Marmann, Healy World GmbH Isaac-Fulda-Allee 1, 55124 Mainz, Germany, Tel: +491718450247
Abstract
Background: The COVID-19 pandemic is one of the major factors in increasing people’s perceived stress level. In previous studies, Individualized Microcurrent Frequency (IMF) devices were shown to be effective in improving participants’ mental status and wellbeing. We hypothesized that specially designed IMF applications would increase the effect in comparison to already es-tablished standard applications as used in participants’ daily routine. Method: Healthy volunteers who had given informed consent were randomized to one of the treatment groups using a set of Power of Three IMF programs, which is specially designed for stress reduction, or using the IMF setting as already established prior to study start. In both groups, perceived stress (Perceived Stress scale, PSS), mental wellbeing (WHO-5 wellbeing questionnaire) and self-assessment of experienced burden (Measure Your Medical Outcome Profile, MYMOP) were measured at baseline and after a 3 week application period. It was assumed that the specially designed application setting would have an additional beneficial effect in comparison to the also effective standard application. Results: Statistical analysis confirmed that the two active interventions were effective in increasing wellbeing and decreasing perceived stress and perceived individual burdens. For all parameters the effect sizes were statistically significantly higher in the study group using the specially designed application setting. Discussion and Conclusion: The Healy IMF short term applications can improve the wellbeing, stress level and anticipated concerns of healthy persons by the two investigated modes of action. Special adaptions of the program setting are improving the effect size. A testing of these applications for long term improvements would be warranted.
Key words: Individualized microcurrent fre-quencies, wellbeing, stress, resilience, healy
Introduction
The term »stress« (lat. strictus: taut) was taken from English and means pressure, strain or tension in the technical-physical context. In everyday theory, stress is usually understood as psychosocial stress and refers to those situations that, for example, cause disorders, irritations and anxiety and contribute to an impairment of mental or physical wellbeing [1].
The COVID-19 pandemic may have brought many changes to how people live their lives, and with it, at times, uncertainty, altered daily routines, financial pres-sures and social isolation. People may worry about getting sick, how long the pandemic will last, whether their job will be affected and what the future will bring. Information overload, rumors and misinformation can make life feel out of control and make it unclear what to do.
The WHO’s Global Burden Disease Study estimated that the COVID-19 pandemic has led to a 27.6% increase (95% uncertainty interval (UI): 25.1–30.3) in cases of major depressive disorder (MDD) and a 25.6% increase (95% UI: 23.2–28.0) in cases of anxiety disorders (AD) worldwide in 2020 [2].
Individualized Microcurrent Frequency (IMF) applica-tions are shown to be effective in the treatment of mental problems [3-5]. Microcurrent may render its effects via rhythmic stimulation that synchronizes and enhances the efficacy of endogenous neurophysiologic activity [6]. Additionally, increases in blood and cerebrospinal fluid levels of specific neurotransmitters, including sero-tonin, norepinephrine, dopamine, and β-endorphin have been reported when microcurrent was used for 1 or 2 weeks [7].
For a great variety of indications, it has been shown that specially designed microcurrent frequency protocols have positive effects on improving the respective conditions. Designing microcurrent protocols in this context means that special frequency patterns are chosen to gain the best effect for the respective condition [8, 9].
It was shown that frequency therapy has positive effects concerning the treatment of depression [10,11], anxiety and associated sleep disorders [12,13] in devic-es using the same mode of action as the investigational product (IP). As a consequence it is expected that IP’s microcurrent frequency application could improve the stress level and general wellbeing in healthy study vol-unteers exposed to corona crisis induced stress.
All participants should document an assessment of their current status of wellbeing (WHO-5Q [14,15]), their major concerns (adapted MYMOP questionnaire [16-19]) and their perceived stress level (PSS [20-22]) before any application of the used IMF programs and after 3 weeks of application. Meanwhile, the control group assesses the changes in wellbeing and the status of their major concerns under normal living conditions and without using the Healy IMF programs.
Vaccine hesitancy, negative attitudes, reluctance or even refusal to be vaccinated may stem from general mistrust in science, conspiratorial attitudes, or overvalued ideas regarding the safety of the vaccine [23]. The perceived stress situation caused by the COVID-19 crisis is considerably different in subjects refusing vaccination in comparison to vaccinated persons. This difference in stress perception may also have some consequences on any stress specific treatment.
Materials and Methods
Design
The study was designed as a two-armed, open, three weeks treatment duration with a measurement point at the beginning and at the end of the study. A study protocol was finalized before commencement of recruitment. Volunteers were recruited via an existing net-work of persons interested in this type of treatment. After signing the online informed consent form, partici-pants were randomly assigned to one of the two study groups:
Application group (A)
Participants who already use the investigational device in daily routine (existing clients); application of two Power of Three Programs designed for stress reduction two times per day for 3 weeks.
Application group (B)
Participants who already use the investigational device in their daily routine (existing clients) and willing to continue using the Healy device according to the established routine during the following 3 weeks of study participation.
Participants
Participants were volunteers who felt moderately stressed and would profit from some self-help treatment in their general wellbeing, coping with particular issues, such as sleep problems, low affect or lack of energy, or in reducing their perceived stress level. They gave informed consent to participate prior to any study specific procedure.
Volunteers were advised to participate only if they would not violate any restrictions for use as given in the device product information (pregnancy, having an implanted pacemaker or any other electronic or metallic device at or near the place of application on the body, open wounds, scar tissue or insensitivity or radiation therapy near the place of application, or a history of epi-lepsy).
Treatment device
For application of individualized frequency modulated microcurrent applications the investigational device (Healy device) is to be attached to the body via electrodes and cables on various places depending on the program and the aim. The electrodes were exclusively placed as conductive bracelet electrodes at the wrists, so that the microcurrent can flow through the upper part of the body.
Healy uses frequencies from 0.1 Hz to 1 MHz. Healy applies an electrical current between 0 µA and 4000 µA. The maximum applied voltage is 10 V.
Treatment application
Participants assigned to group A will apply the Indi-vidualized Microcurrent Frequency (IMF) programs Conflict Balance, Defense Support, Friendly Flora and Re-balance. These programs are especially designed for stress reduction. The programs were applied according to a predefined treatment plan two times per day with one day without any application per week for a total of 3 weeks.
Participants of group B are assigned to use classic Healy applications as already established in the pre-existing freely selected application schedule.
In both groups IMF programs were applied via the bracelet electrodes attached on the parti-cipants’ wrists.
Outcome measures
Due to the deliberately heterogeneous volunteer sample, we opted for one very generic and one very individualistic outcome measure. The primary outcome was the WHO5-Wellbeing scale [14,15], a 5-item scale that has been found to be both very parsimonious, reliable and widely applicable to measure wellbeing as a generic scale. The five items of the scale reflect on the state of the last 2 weeks (cheerful and good spirits, calm and relaxed, active and vigorous, woke up fresh and rested, daily life filled with interesting things) and are rated on a six-point Likert scale (“at no time”, “some of the time”, “less than half of the time”, “more than half of the time”, “most of the time”, “all of the time”). The items can be summed up to yield a sum score ranging from 0 to 25, or, if standardized, on a percentage scale from 0 to 100. Clinically manifest depression is supposed to be present if someone scores less than 50 points, and population means in European countries are around 70 points. We used the standardized sum score as a main outcome and present these standardized scores (sum score multiplied by 4).
As a secondary outcome we used an individualized score, the Measure Your Own Medical Outcome Profile (MYMOP) Score [16-19]. This is an individually defined measurement system following the generic approach of goal attainment scaling [24]. Individuals are free to define as many – usually up to three – areas of their physical or mental state that they want to see changed. This can be, for instance, sleep, energy and mood in one patient, and mobility, pain and sexual interest in another. This way, everyone can choose their own areas of change. It is initially rated on a 10-point numerical rating scale. The content area is safely stored and implemented in the follow-up measurement for the participant to score once more. We used the (one) most important concern that participants could mention and rate it at the beginning and after 3 weeks of treatment.
The third outcome measure was assessed by use of the Perceived Stress Scale (PSS) [20-22], the most widely used psychological instrument for measuring the per-ception of stress. It is a measure of the degree to which situations in one’s life are perceived as stressful. Items were designed to tap how unpredictable, uncontrollable, and overloaded respondents find their lives. The scale also includes several direct queries about current levels of experienced stress. The PSS items are easy to under-stand and the response alternatives are simple to grasp. The questions in the PSS ask about feelings and thoughts during the last month. In each case, respondents are asked how often they felt a certain way.
For the safety assessment, adverse events were que-ried with an open-ended question in the final survey.
Outcomes were measured by presenting the ques-tionnaires as online questionnaires, as soon as informed consent was received, and then again after three weeks, using an email prompting system that led participants to the online questionnaire.
Since the study was conducted with healthy, well-informed volunteers giving informed consent, ethical counsel was not sought and was not necessary according to local legal frameworks.
Statistics
The statistical analysis was performed hierarchically in a 3 step procedure:
1. A pre/post comparison of the different study groups concerning the WHO5-Wellbeing scale, the MYMOP and the Perceived Stress Scale respectively to confirm the efficacy of treatments by use of t-tests for paired samples. H0: no difference between baseline and study completion: Baseline Score = Completion Score within each treatment groups.
H1: increase in wellbeing score, respective decrease in symptom burden score and perceived stress scale during the study: Baseline Score > Completion Score (for wellbeing) respective Baseline Score < Completion Score (for MYMOP Symptom Load and PSS)
2. Covariance analytic methods to confirm superiority of treatment A (specific IMF programs for stress reduction) in comparison to treatment B (standard Healy ap-plication).
H0: No differences between the study groups.
H1: Treatment effect in group A > treatment effect in group B.
3. Sub-group analysis comparing the effects of vac-cination status on perceived stress at baseline and treatment effect on stress reduction.
H0: No differences between subgroups (vaccinated versus not vaccinated within the treatment groups).
H1: Treatment effect in vaccinated participants ≠ treatment effect in unvaccinated participants within each treatment group
All data sets were inspected for violation of the re-quired assumptions to perform parametric tests. In case of any violation of these requirements a non-parametric test would be performed, but all datasets conformed well to normal distribution, homogeneity of variances and no outliers could be detected.
As this was a pilot study, no sample size calculation was conducted. It was assumed that a group size of 300 participants would allow the detection of clinically relevant group differences.
For the wellbeing score and the perceived stress score missing data were to be interpolated by a conservative last-value-carried-forward algorithm which assumes no change between baseline and follow-up. This was only employed for these instruments and if no more than one single data point of a data set was missing. In all other cases (if more than one data point per set was missing), the respective dataset was excluded from the analysis.
As goal attainment (MYMOP) might not be fully com-pleted by some participants and because of its extremely individual nature, it was decided before commence-ment of the actual analysis to not use any missing data interpolations, but to exclude the corresponding partic-ipants from the evaluation.
Safety assessment
All diseases that were reported in the second survey will be grouped according to the MedDRA system organ classes and listed per application group. Incidences of Adverse Events (AEs) per Organ class and group and incidences of AEs assessed as potentially induced by the study procedure will be compared between the two groups.
Results
The study was conducted from December the 14th 2021 (first participant answered the first survey) to February 9th in Germany. This was within the within the 4th Corona-wave with increasing incidences (about 51000 on 15th December 2021 to 250000 on 10th February 2022) [22].
596 participants consented to the study and completed both questionnaires.
284 participants were assigned to the Power of Three group (A) and used twice per day one Healy application of the Power of Three program group; 312 participants were assigned to the standard IMF application group (B) and used the Healy IMF device as before.
As can be seen from table 1, the randomization process yielded two quite similar groups. Due to data protection concerns, age was only collected in broad categories. Most of the participants, 88%, were female. 63% or 386 participants belonged to the middle-aged group between 41 and 60, and nearly 12% were older than 60 years ( Table 1).
Table 1.Gender, Age-Groups, and Reasons for being stressed per group; absolute frequencies and percent-ages (per category and group); compliance per treatment group defined as follows: for the Power of Three group performance of at least 50% of the stipulated applications are defined as compliant, participants of the standard IMF application group were considered as compliant if they had performed at least 10 appli-cations during the 21 days observational period.
| Power of Three group | Standard Healy application | |||||
|---|---|---|---|---|---|---|
| Vaccinated | Not vaccinated | Total | Vaccinated | Not vaccinated | Total | |
| (N = 104) | (N = 180) | (N = 284) | (N = 98) | (N = 214) | (N = 312) | |
| Gender | ||||||
| Female | 89(86%) | 150(83%) | 239(84%) | 89(91%) | 188(88%) | 277(89%) |
| Male | 15(14%) | 30(17%) | 45(16%) | 9(9%) | 26(12%) | 35(11%) |
| Age Groups | ||||||
| <20 | 0(0%) | 0(0%) | 0(0%) | 1(1%) | 1(1%) | 2(1%) |
| 20-40 | 22(21%) | 44(24%) | 66(23%) | 18(18%) | 53(25%) | 71(22% |
| 41-60 | 71(68%) | 115(63%) | 186(65%) | 64(63%) | 136(63%) | 200(63%) |
| 61-80 | 11(11%) | 22 (11%) | 33(11%) | 17(16%) | 24(11%) | 41(13%) |
| Stress was caused by (several answers allowed…) | ||||||
| Worries about family/partnership | 69(66%) | 136(75%) | 205(72%) | 69(70%) | 158 (73%) | 227(73%) |
| Corona Crisis | 68(65%) | 88(48%) | 156(55%) | 59(60%) | 107(50%) | 166(53%) |
| Health concerns | 48(46%) | 60(33%) | 108(38%) | 56(57%) | 85(40%) | 141(45%) |
| Financial uncertainties | 48(46%) | 99(55%) | 147(52%) | 31(32%) | 94(44%) | 125(40%) |
| Losses (human or animal) | 41(39%) | 81(45%) | 122(43%) | 38(38%) | 104(48%) | 141(45%) |
| Others | 38(37%) | 74(41%) | 112(39%) | 32(33%) | 79(37%) | 111(36%) |
| Compliance | ||||||
| Compliant | 79(75%) | 161(89%) | 240(84%) | 77(79%) | 170(79%) | 247(79%) |
| Non-Compliant | 25(25%) | 19(11%) | 44(16%) | 21(21%) | 44(21%) | 65(21%) |
Whereas overall group differences concerning the profiles of stress causing factors are small and not significant (Chi square test p = 0.22), the difference between the vaccinated versus not vaccinated subgroups was more clearly pronounced and significant (Chi square test p = 0.0038).
Regarding the reasons for feeling stressed, the most prominent differences between the vaccinated and not vaccinated subgroups could be seen in the perception of the corona crisis and health concerns as a reason for being stressed. For both study groups, the perception of the respective factor as cause of being stressed was about 15 % higher in the vaccinated subgroup.
Table 2.Baseline values of outcome parameters WH0-5 score, Self-assessment of most important concerns and Perceived Stress Scale, mean values and 95% confidence interval.
| Power of Three group | Standard Healy application | |||||
|---|---|---|---|---|---|---|
| Vaccinated | Not vaccinated | Total | Vaccinated | Not vaccinated | Total | |
| (N = 104) | (N = 180) | (N = 284) | (N = 98) | (N = 214) | (N = 312) | |
| WHO-5 Score | 31,65 | 33,90 | 33,07 | 33,54 | 35,20 | 34,66 |
| [28,39 – 34,91] | [31,13 – 36,67] | [30,96 – 35,19] | [29,92 – 37,16] | [32,96 – 37,45] | [32,76 – 36,58] | |
| Concern (MYMOP) | 8,09 [7,78 – 8,39] | 8,31 [8,09 – 8,52] | 8,23 [8,05 – 8,40] | 7,82 [7,51 – 8,13] | 8,14 [7,95 – 8,33] | 8,04 [7,87 – 8,20] |
| Perceived Stress (PSS) | 23,49 [22,35 -24,62] | 22,54 [21,70 -23,40] | 22,89 [22,22 -23,57] | 22,21 [21,02 -23,40] | 23,00 [22,24 -23,75] | 22,74 [22,10 -23,38] |
The baseline outcome data were similarly evenly dis-tributed, with also equally very small differences within the different subgroups.
The testing procedure using t-Test for paired samples yielded a highly significant increase of the WHO-5 scores for both treatment groups using the Power of Three application respective the standard Healy application during the treatment phase by about 25.8 (Power of Three), respective 19.1 (standard IMF) scoring points (t = -20.638, df = 279, p-value < 2.2e-16 for group A; t = -18.894, df = 311, p-value < 2.2e-16) (Figure 1). The group difference in effect size respective increase in wellbeing score was highly significant (t = 4.2258, df = 590, p-value = 0.00001379).
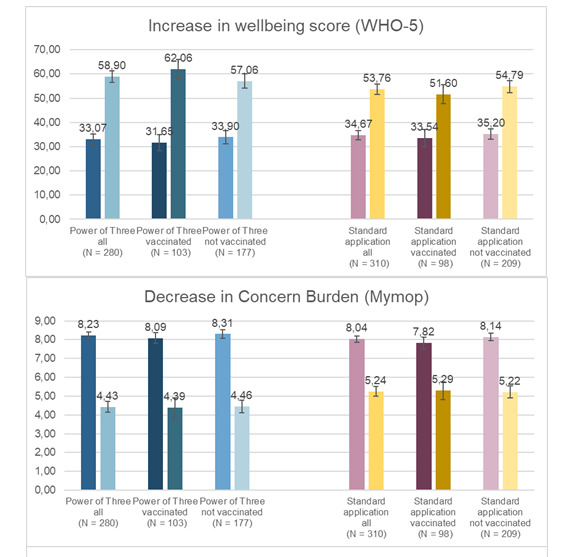
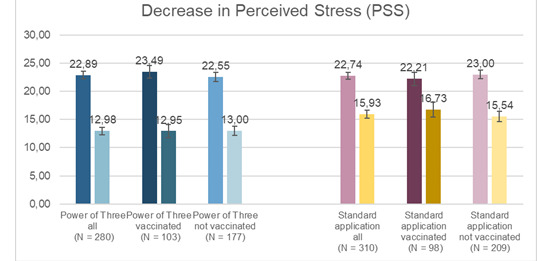
Figure 1:Increase in Wellbeing score (WHO-5), decrease in Concern-burden (MYMOP) and decrease in stress level (PSS) in both treatment groups, first column baseline, second column final assessment. Mean values and 95% confidence intervals
The same patterns as found for the Wellbeing score could also be detected for the decrease in concern burden and decrease in perceived stress. Pre-post compari-sons yielded highly significant decreases of stress level and concern burden in both treatment groups and a significant higher effect size was present under Power of Three application than under standard Healy applica-tion. The results of the statistical test performed are summarized in Table 3.
Table 3.Results of the statistical test Pre/post differences of the respective parameter (paired t-test) and group comparison of the respective effect size (Covariance analysis with baseline adjustment)
| Parameter | Pre/Post Comparison, Power of Three Group (paired t-test) | Pre/Post Comparison, standard Healy application Group (paired t-test) | Group Comparison of respective effect size (Covariance analysis with baseline adjustment) |
|---|---|---|---|
| Wellbeing | Mean of the differences = 25.82857; t = 20.638, df = 279, p-value < 2.2e-16 | Mean of the differences = 19.08974; t = 18.894, df = 311, p-value < 2.2e-16 | Df = 1 F =17.299 p = 0.00003669 |
| Concern-burden | Mean of the differences = 3.796429; t = 25.413, df = 279, p-value < 2.2e-16 | Mean of the differences = 2.809677 t = 19.022, df = 309, p-value < 2.2e-16 | Df = 1 F = 19.707 p = 0.000010784 |
| Stress relief | Mean of the differences = 9.910714 t = 26.26, df = 279, p-value < 2.2e-16 | Mean of the differences = 6.814103 t = 18.877, df = 311, p-value < 2.2e-16 | DF = 1; F = 11.168 p = 0.0008848 |
For sub-group analysis (comparison of vaccinated versus not vaccinated participants), a two-factorial analysis of variance with the two factors treatment group and vaccination status was performed for each of the parameters.
For stress relief and increase of wellbeing the interac-tion between the two factors was significant (df = 1, F = 7.4019 p = 0.006708 for stress relief and df = 1, F = 6.9327 p = 0.008686 for wellbeing) whereas for the vaccination status per se no significant effect could be de-tected (df = 1, F = 1 0.8457 p = 0.358149 for stress relief and df = 1, F = 2.9150 p= 0.088287 for wellbeing).
Concerning concern burden, only marginal differences could be observed in the comparison of the subgroups of vaccinated participants versus non vaccinated partic-ipants (Figure 1). Two-factorial analysis of variance resulted in significant group differences (df = 1 F = 21.0236 p = 0.00000554), whereas both, vaccination status (df = 1, F = 1.1626, p = 0.2814) and interaction between group and vaccination status (df = 1 F = 0.6986, p = 0.4036) are not significant.
Safety assessment
Altogether 157 individuals reported in total 168 ad-verse issues. None of these AEs fulfilled a condition of being a serious adverse event. 96 Adverse events oc-curred in participants assigned to group A (Power of Three), 72 in participants of group B (standard Healy appli-cation).
24 adverse events were assessed as related to the study procedures (10 in group A and 14 in group B). Most frequent adverse events related to investigational procedure are pain (10 cases, 5 in each group), side effects of detoxification (1 in each group) and infections (1 in each group). Beside this, reduced eyesight, low blood pressure and dizziness (in group A), exhaustion, skin itching, difficulties breathing, sleep disorder, depression, gastrointestinal complaints and migraine (in group B) were reported once as an event related to the investigational procedure. The frequencies of adverse events in different system organ classes according to MedDRA classification are given in table 4.
Table 4.Incidence of AEs occurring during the study according to MedDRA SOCs.
| MedDRA System Organ class | Group A (Power of Three) | Group B (standard Healy application) |
|---|---|---|
| Infections and infestations | 31 | 23 |
| Musculoskeletal and connective tissue disorders | 17 | 11 |
| Nervous system disorders | 10 | 7 |
| Gastrointestinal disorders | 6 | 6 |
| Skin and subcutaneous tissue disorders | 7 | 2 |
| Product issues | 4 | 6 |
| Respiratory, thoracic and mediastinal disorders | 5 | 2 |
| Psychiatric disorders | 4 | 2 |
| Renal and urinary disorders | 2 | 3 |
| Ear and labyrinth disorders | 2 | 2 |
| Eye disorders | 2 | 1 |
| Injury, poisoning and procedural complications | 1 | 2 |
| Vascular disorders | 0 | 3 |
| General disorders and administration site conditions | 1 | 1 |
| Cardiac disorders | 1 | 0 |
| Endocrine disorders | 0 | 1 |
| Metabolism and nutrition disorders | 1 | 0 |
| Immune system disorders | 1 | 0 |
| Surgical and medical procedures | 1 | 0 |
Discussion
In this randomized non blinded study, we compared the efficacy of a new, designed especially for stress reduction IMF application setting with an active control group, of participants using IMF applications according to their previously established routine. The intention of this design was to determine the additional benefit of adapting an effective treatment (standard IMF) to special conditions.
We chose 3 different well established instruments measuring different components of a participant’s stress perception and its influence on the awareness of impairment of living condition; the WHO-5 quality of life questionnaire assessing the subjective psychological wellbeing [20], the Measure Yourself Medical Outcome Profile (MYMOP) modified for non-medical conditions to measure the participants’ perception of the most important stressing factor and the ‘Perceived Stress Scale’ to measure the degree to which situations in one’s life are perceived as stressful. Psychological stress has been defined as the extent to which persons perceive (appraise) that their demands exceed their ability to cope.
Assessment results of all these 3 instruments are influenced by both the participants’ internal perception and by external factors like changes in the external setting (stress inducing situations). In this study the corona situation in Germany was the most dominant external factor causing participants to feel stressed. The study was conducted in a period with increasing incidences of Corona infections (increasing period of the 4th Corona Wave) and more restricting regulations by the gov-ernment. A positive effect of this external setting on the parameters measured in the course of the study could be ruled out.
The results of this pilot study are indicating clear evi-dence for the efficacy of IMF treatment in improving the wellbeing of stressed subjects. The baseline values for PSS were about 10 points higher than comparative means of the population before the corona pandemic [19]. The WH0-5 wellbeing scores were about 35 points lower than population comparisons before the corona pan-demic [23]. In both application groups scores improved towards mean values of comparative populations under pre-corona conditions.
For the MYMOP questionnaire, comparative data from the literature are missing. Yet for this parameter there was also a marked improvement in concern burden over the course of the study; by 3.8 for the Power of Three group and by 2.8 for the comparison group.
For all parameters, the Power of Three group was significantly superior to the comparison group (standard IMF). The calculation of the effect size (Cohen’s d) for the added benefit of the specially adapted treatment compared to the standard IMF treatment results in values that are in the range of small effects [27,28] (0.348 for WHO-5, 0.488 for PSS, 0.370 for MYMOP) but for all these are different from 0. This indicates that the additional benefit of specially designed IMF programs in stress reduction is small, but significant.
Several recent independently performed meta-analyses on the effect of the so-called placebo effect showed that there is little reliable evidence that the pla-cebo effect can play a role in curing or controlling disease by modifying pathophysiology [29-32]. Contrary to this generalized implication, it was shown in some studies that the mind-body interaction triggered by placebo interventions could produce changes in both symptoms and pathophysiology [33-36]. If this was also the case in our study, this means that even blinding would not allow to separate between the direct effect of the treatment and the effect mediated throughout the participants’ expectations. However, in our view, for practical purposes this separation is artificial, for in each treatment situation in the real world psychological and genuine treatment effects are mixed and very likely act synergistically to enhance each other [37]. It seems rather interesting that a short term treatment can elicit clinically meaningful effects on stress reduction.
There was a significant difference in the assessment of stress inducing factors between the subgroups of vaccinated and non-vaccinated participants. For non-vaccinated participants the corona situation and health concerns are less important as stress inducing factors than for vaccinated participants. Despite this fact, only minor differences could be detected respective improv-ing in wellbeing or reduction in concern burden and stress level between both subgroups. So, vaccination status may have had only a minor influence on the study results.
The proportion of participants who experienced at least one health impairment in the course of the study is comparatively high at 26%. This may be because the study was conducted in the winter period and that the study participants were exposed to a high level of stress. Both factors are associated with high rates of health impairments [38,39]. None of the documented conditions were severe. 4% of the health impairments were assessed as related to the IMF application by the study partic-ipants themselves. In most cases these impairments were assessed as temporary adaptations to new programs (6 cases) or caused by too high intensities of applied current (5 cases). The symptoms disappeared in the course of the study or after decreasing the application intensity.
Conclusion
As already demonstrated in other studies [3-5,40-42], IMF application is efficient, safe and well tolerated by users and highly efficient in improving wellbeing and stress perception. This effect could even be significantly improved by the application of specially designed fre-quency protocols and application schedules.
Abbreviations
AE: Adverse Event; AD: Anxiety Disorders; Covid: Co-rona Virus Disease; Hz: Hertz; IMF: Individualized Microcurrent Frequency; IP: Investigational Product; MDD: Major depressive disorder; MedDRA: Medical Dictionary for Regulatory Activities; MHz: Mega Hertz; µA= Milli Ampere; MYMOP: Measure Yourself Medical Outcome Profile; PSS: Perceived Stress Scale; SOC: System Organ Class; UI: uncertainty interval; V: Volt; WHO: World Health Organization.
Acknowledgements
We are grateful to the participants that they helped in this research by participating without remuneration.
Authorship statement
Dr. Peter Marmann (PM) organized the study, recruited the participants and collected the data. He also analyzed the data and wrote the first draft of the manuscript.
Marcus Schmieke (MS) developed the design of the study and finalized the manuscript.
Sponsoring
The study was sponsored by Healy GmbH, Kränzlin, Germany.
Role of the sponsor
The sponsor helped with recruitment by activating his network of users and paid for the analysis. The sponsor suggested some aspects of the design, like the two active modes of action, superiority of both active groups against the untreated control group. He paid for the costs of the study and the analysis.
Ethics Statement
As this study was performed with healthy volunteers who were fully informed and gave written informed consent, there was no legal requirement to seek ethical clearance and as the potential benefit – receiving a program group for free – outweighed the risks, which is non-existent, we felt that ethical clearance was unnecessary.
Informed consent statement
Written informed consent has been obtained from the participants(s) to publish this paper prior to any study related procedure. All data have been pseudonymized prior to evaluation.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Conflict of interest
The author has the following conflict of interests: The Author Dr. Peter Marmann is an employee of Healy GmbH, the sponsor of the study.
References
1. Plaumann M, Busse A, Walter U. Grundlagen zu Stress. In: Weißbuch Prävention. 2005/2006; 2005:20. Springer, Berlin, Heidelberg. https://doi.org/10.1007/3-540-32662-6_2
2. Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxi-ety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
3. H. Walach, P. Marmann. Self-Treatment to Improve Mental and Physical Health using Two Bioenergetic Devices: A Randomized Controlled Trial. Journal of Psychiatry and Psychiatric Disorders 5 (2021):107-119.
4. Schmieke, Marcus. (2021). Quantum En-tangled Frequencies and Coherence in Bioenergetic Systems: Information Field Processes related to the Concepts of Akasha and Prana. Dev Sanskriti Interdisciplinary International Journal. 18. 10-33. 10.36018/dsiij.v18i.226.
5. Sharp SJ, Huynh MT, Filart R. Frequency-Specific Microcurrent as Adjunctive Therapy for Three Wounded Warriors. Med Acupunct. 2019 Jun 1;31(3):189-192. doi: 10.1089/acu.2019.1366. Epub 2019 Jun 17. PMID: 31297172; PMCID: PMC6604905.
6. Zaghi S, Acar M, Hultgren B, Boggio PS, Fregni F (2009) Noninvasive brain stimulation with low-intensity electrical currents: putative mecha-nisms of action for direct and alternating current stimulation. Neuroscientist
7. Millet B. Les techniques par électrostimu-lation dans le traitement des dépressions sévères [Electrostimulation techniques in treatment for se-vere depression]. Encephale. 2009 Dec;35 Suppl 7:S325-9. French.
8. McMakin, C., Oschman, J L The Resonance Effect: How Frequency Specific Microcurrent Is Changing Medicine (Paperback); Publisher: North At-lantic Books,U.S. ; ISBN: 9781623171100, 19/04/2017
9. Mercola, Joseph M., and Daniel L. Kirsch. The basis for microcurrent electrical therapy in conventional medical practice. Journal of Advancement in medicine 8, no. 2 (1995): 107-120.
10. Shealy CN, Cady RK, Culver-Veehoff D, Cox R, Liss S (1998) Cerebrospinal fluid and plasma neurochemicals: response to cranial electrical stimulation. J Neurol Orthop Med Surg 18(2):94–97
11. Barclay TH, Barclay RD. A clinical trial of cranial electrotherapy stimulation for anxiety and comorbid depression. Journal of Affective Disorders. 2014; 164: 171‐177. Presented at the American Psychological Association National Conference, Hono-lulu, HI, July 2013.
12. The Alpha-Stim 100 Product information: Electromedical Products International, Inc. 2201 Garrett Morris Parkway Mineral Wells, Texas 76067-9034 USA.
13. Yennurajalingam S, Kang D‐H, Hwu W‐J, et al. Cranial electrotherapy stimulation for the management of depression, anxiety, sleep disturbance, and pain in Participants with advanced cancer: a preliminary study, Journal of Pain and Symptom Management. E‐published ahead of print, September, 2017.
.14. Christian Winther Topp, Søren Dinesen Østergaard, Susan Søndergaard, et al. The WHO-5 Wellbeing Index: A Systematic Review of the Litera-ture. Psychother Psychosom. 2015; 84:167–176
15. Bech P, Olsen L, Kjoller M, et al. Measuring wellbeing rather than the absence of distress symptoms: a comparison of the SF-36 Mental Health subscale and the WHO-Five Wellbeing Scale. Int J Methods Psych Res. 2003; 12:85-91.
16. Kiresuk TJ, Sherman R. Goal attainment scaling: general method for evaluating comprehensive community mental health programs. Community Ment Health J. 1968; 4: 443-53.
17. Klein EM, Brähler E, Dreier M, et al. The German version of the Perceived Stress Scale - psychometric characteristics in a representative Ger-man community sample. BMC Psychiatry. 2016;16:159.
18. Hermann K, Kraus K, Herrmann K, et al. A brief patient-reported outcome instrument for primary care: German translation and validation of the Measure Yourself Medical Outcome Profile (MYMOP). Health and quality of life outcomes. 2014;12(1):112.
19. Hermann K, Kraus K, Herrmann K, et al. A brief patient-reported outcome instrument for primary care: German translation and validation of the Measure Yourself Medical Outcome Profile (MYMOP). Health Qual Life Outcomes. 2014, 12: 112
20. Cohen S, Kamarck T, Mermelstein R A global measure of perceived stress. Journal of Health and Social Behavior. 1983; 24, 386-396.
21. Cohen S, Williamson G. Perceived Stress in a Probability Sample of the United States. Spacapan, S. and Oskamp, S. (Eds.) The Social Psychol Health. Newbury Park, CA: Sage, 1988.
22. Schneider, Eva Elisa, Schönfelder, Sandra, et al. Measuring stress in clinical and nonclinical subjects using a German adaptation of the Perceived Stress Scale. Int J Clin Health Psych.
23. Palgi Y, Bergman YS, Ben-David B, Bodner E. No psychological vaccination: Vaccine hesitancy is associated with negative psychiatric outcomes among Israelis who received COVID-19 vaccination. J Affect Disord. 2021; 287:352-353. doi: 10.1016/j.jad.2021.03.064.
24. Paterson C. Measuring outcomes in pri-mary care: a patient generated measure, MYMOP, compared with the SF-36 health survey. Bmj. 1996;312(7037):1016-20.
25. Robert Koch Instiut, Fallzahlen und Meldungen (Stand: 29.8.2022) - RKIhttps://www.rki.de
26. Philipp E. Sischka, Andreia P, et al. The WHO-5 wellbeing index a validation based on item response theory and the analysis of measurement invariance across 35 countries, J Affective Disorders Rep. 2020; 1: 2666-9153, https://doi.org/10.1016/j.jadr.2020.100020
27. Cohen J. Statistical power analysis for the behavioral sciences (2. Auflage). 1988; Hillsdale, NJ: Erlbaum.
28. D Lakens. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. 2013; Cognition. https://doi.org/10.3389/fpsyg.2013.00863
29. Kirsch I. Placebo Effect in the Treatment of Depression and Anxiety. Front Psych. 2019; 10:407.
30. Benedetti F. Placebo Effects: Understand-ing the Mechanisms in Health and Disease. Oxford: Oxford University Press; 2009.
31. Tavel, Morton. The Placebo Effect: The Good, the Bad, and the Ugly. The Am J Med. 2014;127. 10.1016/j.amjmed.2014.02.002.
32. Kirsch I. The emperor’s new drugs: ex-ploding the antidepressant myth. New York: basic books (2010).
33. Reingard BK, Rohrbock MD, Hammer J, et al. Acupuncture has a placebo effect on rectal perception but not on distensiblity and spatial summa-tion: a study in health and IBS. Am J Gastroentroenterol. 2004; 99:1990–1997.
34. Colloca L, Benedetti F, Porro CA. Experi-mental designs and brain mapping approaches for studying the placebo analgesic effect. Europ J Ap-plied Physiol. 2008; 102:371–380.
35. Seegers JC, Lottering ML, Joubert AM, et al. A pulsed DC electric field affects P2-purinergic receptor functions by altering the ATP levels in in vitro and in vivo systems. Med Hypotheses. 2002;58(2):171-6.
36. M von Wernsdorff, M Loef, B Tuschen-Caffier, et al. "Effects of open-label placebos in clinical trials: a systematic review and meta-analysis," Scientific Rep. 2021; 11: 3855.
37. H Walach. "Placebo controls: historical, methodological and general aspects". Philosophical Transactions of the Royal Soci Biological Sci. 2011; 366:1870-1878.
38. Der Informationsdienst des Instituts der deutschen Wirtschaft Der Krankenstand in Deutschland - iwd.de, https://www.iwd.de/artikel/krankenstand-in-deutschland-498654/ 2022
39. Salleh MR. Life event, stress and illness. Malays J Med Sci. 2008;15(4):9-18. PMID: 22589633; PMCID: PMC3341916.
40. Zimmerman, Stephen I, Lerner, et al. Bio-feedback and electromedicine reduce the cycle of pain spasm pain in low back Participants. Med Elec-tronics. 1989; 117: 108‐120
41. Heffernan, Michael. The effect of variable microcurrents on EEG spectrum and pain control. Canadian J Clin Med . 1997; 4(10): 4‐11.
42. Muehsam D, Chevalier G, Barsotti T, et al. An Overview of Biofield Devices. Global adv health med. 2015; 4(Suppl), 42–51. https://doi.org/10.7453/gahmj.2015.022.suppl
Received: August 15, 2022;
Accepted: September 26, 2022;
Published:September 28, 2022 .
To cite this article : Schmieke M, Marmann P. Two Arm Stratified Pilot Study to Assess the Efficacy of the New Individualized Microcurrent Frequencies (IMF) Programs “Power of 3” in Comparison with Standard Healy Applications in Participants Under COVID-19 Crisis Induced Stress. Health Education and Public Health. 2022; 5(2): 508-516. doi: 10.31488/HEPH.179.
© 2022 Schmieke M, et al.